
Summary of:
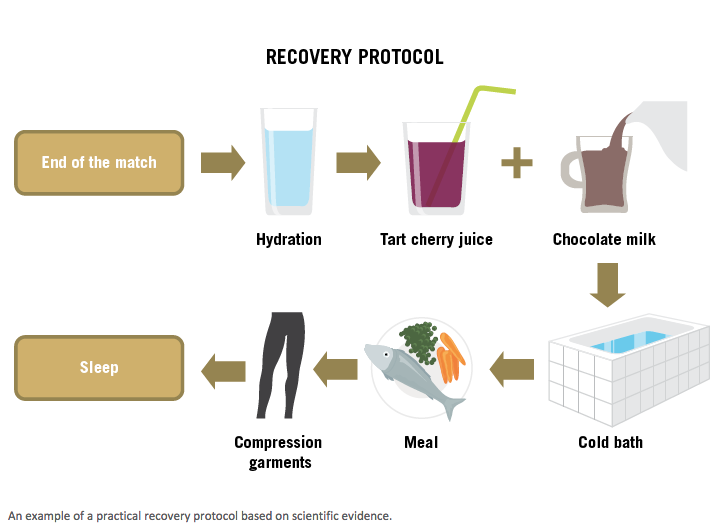
FOOTBALL RECOVERY STRATEGIES (Grégory Dupont, Mathieu Nédélec, Alan McCall, Serge Berthoin and Nicola A. Maffiuletti, 2015) Does Fatigue Cause injury?
|


 | Often when I’m talking to my patient about their injury and why it has happened, they guiltily report that they don’t stretch enough. We’ve all grown up being told how important is it to stretch:
|
I’d guess that most people feel guilty about not stretching enough.
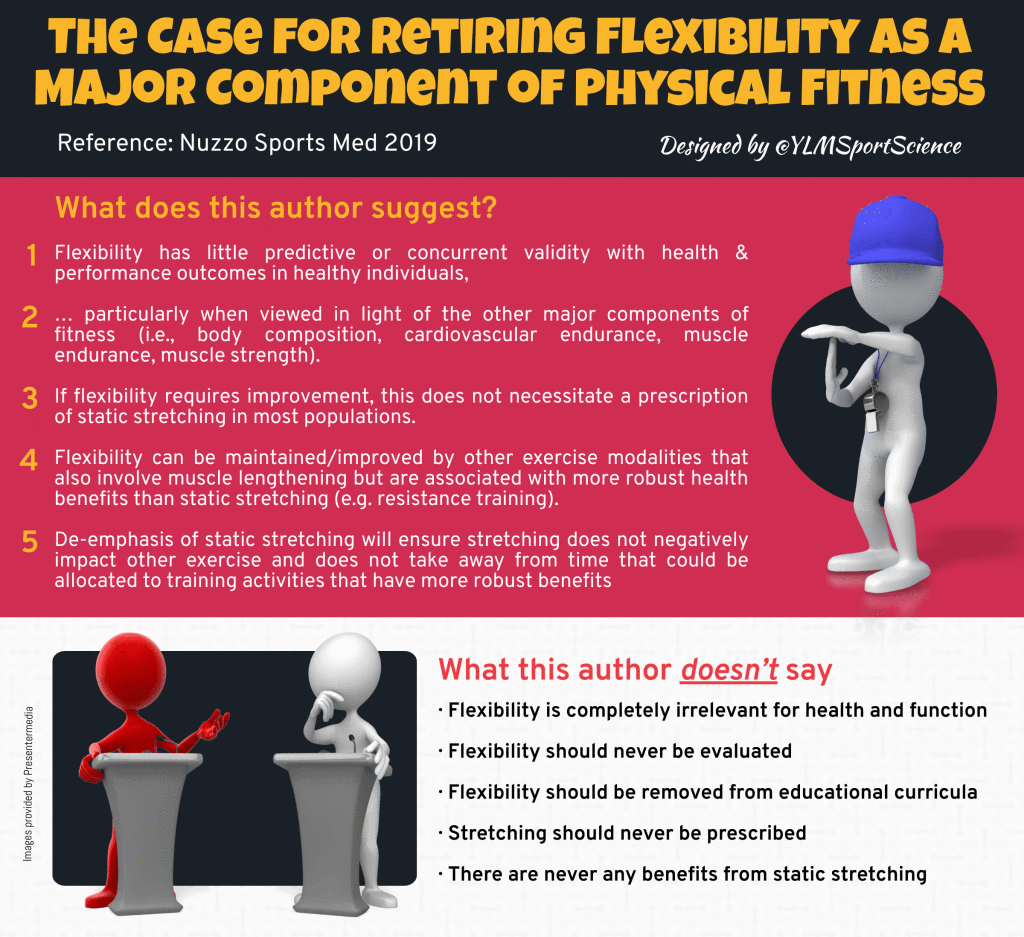
Interestingly, health professionals have changed our tune about the importance of stretching. Research over the last 15 years has suggested static stretching is not as beneficial as was once thought. I’ve been having conversations about the reasons to stretch (or not) for at least the last 15 years, but the current science on stretching just isn’t catching on.
So, what do we know?…
Interestingly, health professionals have changed our tune about the importance of stretching. Research over the last 15 years has suggested static stretching is not as beneficial as was once thought. I’ve been having conversations about the reasons to stretch (or not) for at least the last 15 years, but the current science on stretching just isn’t catching on.
So, what do we know?…
DOES STRETCHING PREVENT INJURIES?
No. There is a lot of evidence that stretching does not reduce the risk of injury. This systematic review and meta-analysis of randomised controlled trials found stretching does not prevent injuries, whether done before or after training. This randomised controlled trial, and this systematic review concluded stretching before exercising only reduces the risk of injury by less than 1%.
Therefore, in practical terms the average athlete would need to stretch for 23 years to prevent one injury. Definitely not worth it.
Therefore, in practical terms the average athlete would need to stretch for 23 years to prevent one injury. Definitely not worth it.
DOES STRETCHING HELP MUSCLE SORENESS?
No. A systematic review concluded that stretching before or after exercising does not confer protection from muscle soreness (ref). Stretching was found to reduce muscle soreness by a trivially small amount - less than 2%.
“Most athletes will consider effects of this magnitude too small to make stretching to prevent later muscle soreness worthwhile.”
DOES STRETCHING INCREASE RANGE OF MOVEMENT?
No. Stretching for the amount of time that most people would hold their stretches, does not make any actual difference to flexibility. The mechanisms of stretching have been extensively studied. There is moderate evidence from a systematic review that stretching can increase flexibility (ref). However, to achieve an actual improvement in muscle compliance we know the total duration of stretching needs to be at least five minutes per muscle group (ref). Therefore to stretch hamstrings, quads, and calves, both left and right, as part of a warm up before sport, it should take at least 30 minutes - which is practically impossible as part of a warm up. We know the one or two, thirty second stretches the majority of athletes would perform during their warm up are just not enough to actually improve their flexibility (ref).
DOES STRETCHING HELP PERFORMANCE?
What people find most surprising about static stretching is it impairs subsequent performance (ref).
A substantial body of research has shown that sustained static stretching acutely decreases muscle strength and power (ref). Stretching before an endurance event lowers endurance performance and increases the energy cost of running (ref). Cycling efficiency and time to exhaustion are reduced after static stretching (ref).
Pretty much any measure of performance is made worse by stretching. Static stretching impairs:
A comprehensive review (ref) from 2011 concludes:
A substantial body of research has shown that sustained static stretching acutely decreases muscle strength and power (ref). Stretching before an endurance event lowers endurance performance and increases the energy cost of running (ref). Cycling efficiency and time to exhaustion are reduced after static stretching (ref).
Pretty much any measure of performance is made worse by stretching. Static stretching impairs:
- strength
- maximal voluntary contraction
- isometric force
- isokinetic torque
- one repetition maximum lifts
- power
- vertical jump
- sprint times
- running economy
- agility
- balance
A comprehensive review (ref) from 2011 concludes:
“Based on the majority of the literature, it would seem logical to recommend that prolonged static stretching not be performed prior to a high level or competitive athletic or training performance.”
WHAT ABOUT DYNAMIC STRETCHING?
Obviously, I’ve been talking about sustained, static stretching. It has been shown that there is no stretch-induced strength loss with dynamic stretching (ref). However, the efficacy of dynamic stretching for increasing flexibility is yet to be determined (ref).
SO WHY STRETCH?
I do get people to stretch if there’s a specific pathology that needs treating. And you do need to stretch if you need flexibility to achieve certain positions in your sporting performance (hurdlers / gymnasts / divers, etc).
SO SHOULD WE STOP STRETCHING?
If you’re happy with your stretching routine, keep doing it. If you think it feels good to stretch after exercise then there’s no harm. But I definitely wouldn’t recommend stretching at the expense of other techniques that are proven to aid recovery.

- Will introducing independent doctors at games help the AFL tackle its concussion problem? -
- The unstoppable rise of the carbon-fibre super shoe -
- Muscle building and resistance training often get ignored, but they're likely to help us age better -
- Evidence doesn't support spinal cord stimulators for chronic back pain -
- Surgery won't fix my chronic back pain, so what will? -
- Can a good night's sleep protect collision sport athletes against concussion? -
- Beetroot isn't vegetable Viagra. But here's what else it can do -

- New research suggests intermittent fasting increases the risk of dying from heart disease -
- AFL considers independent doctors at games to help assess head knocks -
- The role of the physiotherapist in concussion in sport -
- Six tips for sticking to your fitness goals -
- How Cold Weather Saps Your Endurance -
- Esports, pickleball and obstacle course racing are surging in popularity - what are their health benefits and challenges? -


- Football codes' lack of response to AIS concussion guidelines leaves players in limbo for 2024 season -
- Insufficient Evidence for Load as the Primary Cause of Nonspecific Chronic Low Back Pain -
- Does playing football really increase the risk of knee osteoarthritis? -
- AFL changes concussion guidelines for community football but elite level protocols stay the same -
- Gabrielle is hesitant to return to sport after an ACL injury -

Most injuries can be managed with strength training and modifying aggravating activities.
Some pain or discomfort during exercise is OK and safe. It is a good sign if your pain warms up as you exercise and doesn’t feel worse the next day.
KEEP MOVING
Resting too much can be more aggravating than staying active. Reduce your training volume enough to settle symptoms and ensure you don’t feel worse the next day.
PLAN AHEAD
Avoid consecutive days of impact exercise (like running and jumping) if you are sore.
/ Sunday / - / Tuesday / - / Thursday / - / Saturday /
MONITOR MORNING STIFFNESS & SYMPTOMS
Low and stable symptoms are OK. A spike in stiffness, tightness, or pain, means you’ve probably overdone it the day before. You don’t need complete rest. Continue resistance training, do less impact training.
BE PATIENT
There’s no quick fix.
GENERAL HEALTH
We also need to consider general health variables that contribute to recovery:
Some pain or discomfort during exercise is OK and safe. It is a good sign if your pain warms up as you exercise and doesn’t feel worse the next day.
KEEP MOVING
Resting too much can be more aggravating than staying active. Reduce your training volume enough to settle symptoms and ensure you don’t feel worse the next day.
PLAN AHEAD
Avoid consecutive days of impact exercise (like running and jumping) if you are sore.
/ Sunday / - / Tuesday / - / Thursday / - / Saturday /
MONITOR MORNING STIFFNESS & SYMPTOMS
Low and stable symptoms are OK. A spike in stiffness, tightness, or pain, means you’ve probably overdone it the day before. You don’t need complete rest. Continue resistance training, do less impact training.
BE PATIENT
There’s no quick fix.
GENERAL HEALTH
We also need to consider general health variables that contribute to recovery:
- Nutrition
- Hydration
- Stress
- Sleep
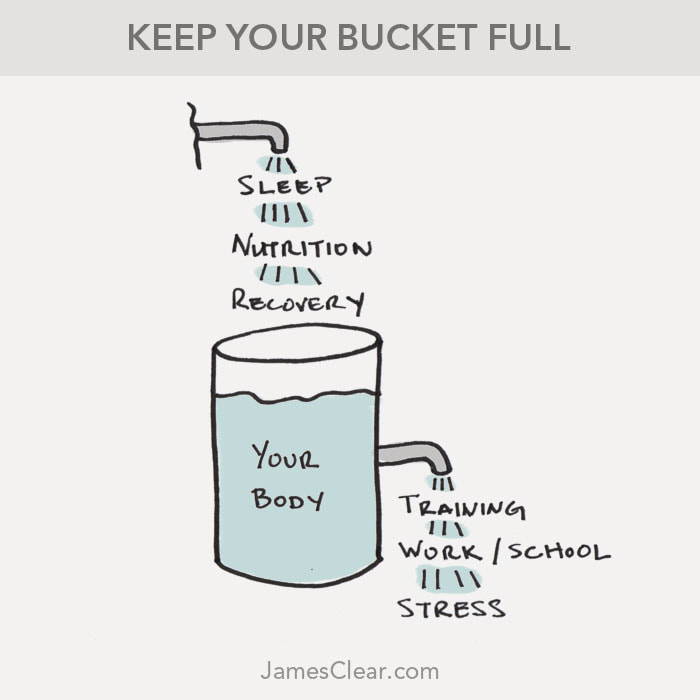
Bucket Image: James Clear - https://jamesclear.com/cumulative-stress
A recently published article by Haroy et al, in the British Journal of Sports Medicine, described a simple exercise routine that decreased the number of groin injuries in male footballers by 41%.
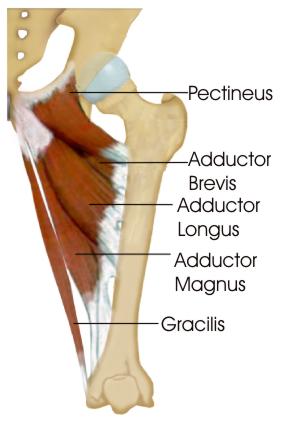
Groin injuries are very common in football. Research shows that weaker groin muscles are associated with an increased risk of groin muscle injury. So strengthening groin muscles can potentially prevent injury.
The paper studied the Copenhagen Adduction exercise, which has previously been shown to strongly recruit adductor longus.
Groin injuries are very common in football. Research shows that weaker groin muscles are associated with an increased risk of groin muscle injury. So strengthening groin muscles can potentially prevent injury.
The paper studied the Copenhagen Adduction exercise, which has previously been shown to strongly recruit adductor longus.
Haroy et al, offered the Copenhagen at three levels of resistance, based of the players’ pain. Players started with Level 3. If the exercise gave them more than 3/10 pain, they were instructed to do the exercise level below instead: 3 > 2 > 1.
| LEVEL 3 VIDEO | LEVEL 2 VIDEO | LEVEL 1 VIDEO |
The training protocol is shown in the following table:

Being only one, quick exercise, compliance was high. They found performing the Copenhagens decreased the risk of groin injury by 41%.
The full article is HERE.
Copenhagens are definitely worth adding to your training. The concept is similar to strengthening hamstrings with the Nordic Hamstring Curl which has been shown to prevent 70%-85% of hamstring strain injuries.
The full article is HERE.
Copenhagens are definitely worth adding to your training. The concept is similar to strengthening hamstrings with the Nordic Hamstring Curl which has been shown to prevent 70%-85% of hamstring strain injuries.
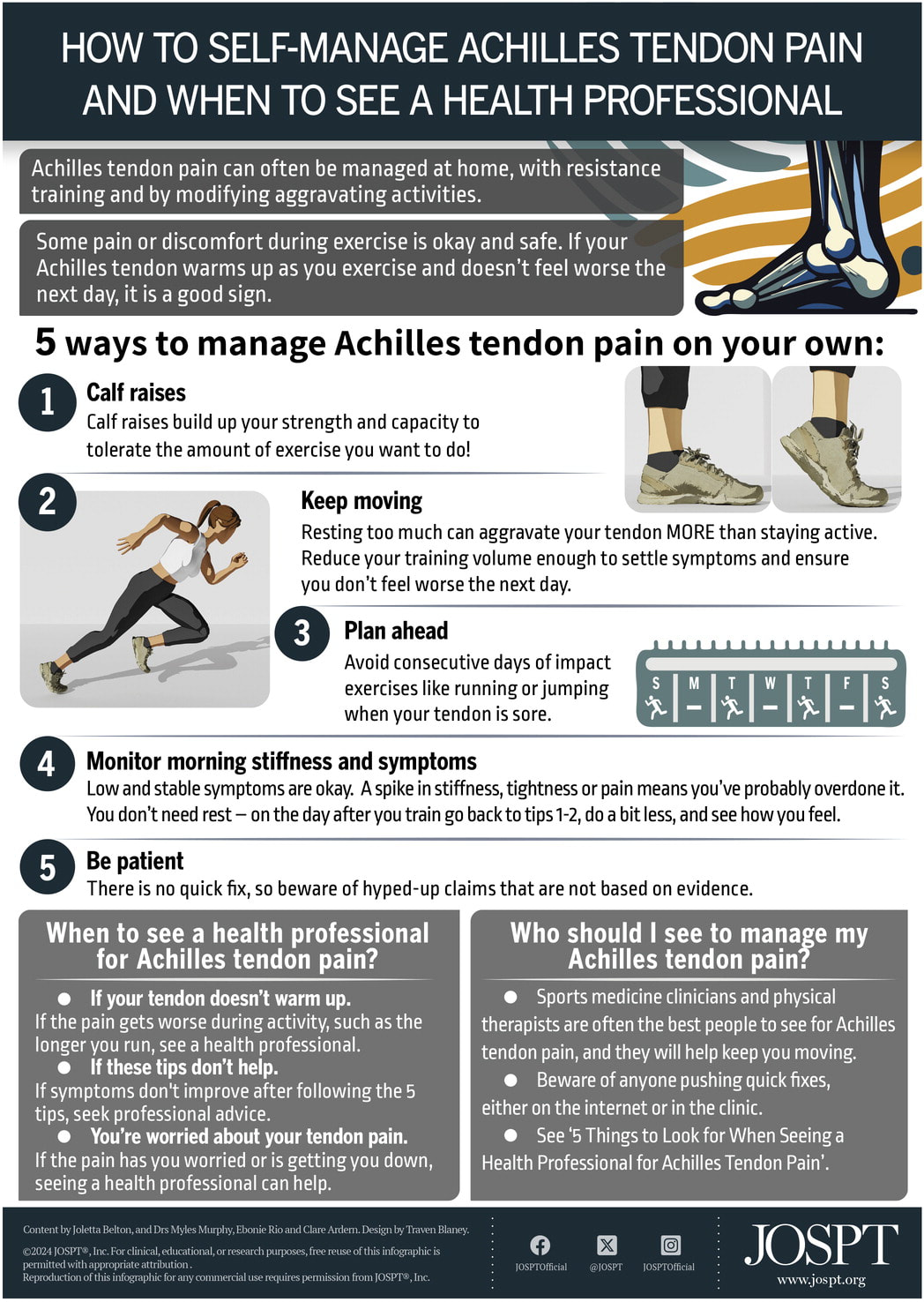
When the Achilles tendon begins to feel painful, two common questions people ask is “what should I do to make it feel better?” and “when should I see a healthcare provider for assistance?”. This infographic guides people with Achilles tendon pain on how they can self-manage their pain and symptoms, plus tips on when to seek professional advice for tendon pain.
J Orthop Sports Phys Ther 2024;54(1):95. doi:10.2519/jospt.2023.9001
J Orthop Sports Phys Ther 2024;54(1):95. doi:10.2519/jospt.2023.9001
|
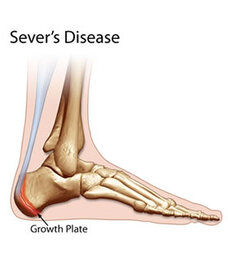
My kids play a lot of sport. When they over-train they get heel pain. Heel pain in kids is called Sever’s disease, or calcaneal apophysitis (which means inflammation of the growth plate of the heel bone - which is the calcaneus). |
HEEL PAIN IN CHILDREN
Sever’s is most common in 9 - 12 year olds. It’s sore to squeeze the bone at the base of the Achilles where it attaches onto the heel. It’s not something that can be seen - it never seems to look red or swollen. It’s worse after sprinting, jumping, and hopping. It settles with rest. It is an overuse injury so it’s common in pre-season, or anytime training loads increase too quickly. My kids get it when they do extra sessions in running spikes or footy boots, without the normal heel support of their running shoes. It’s an overuse injury from excessive loads.
OVERUSE INJURY
When we talk about excessive loads it can be “external” load such as:
I think the running pace is the more powerful multiplier in this list. Extra sprint sessions will do it. My kids got sore once when we did a boot-camp session with a novel plyometric exercise - split jumps.
There are also “internal” variables that determine our ability to cope with the training load:
My kids definitely are more prone to Sever’s if they’ve had a couple of late nights that week. And, if they’re having a growth spurt, their bodies are busy spending resources on growing rather than recovering from the stress of a training session.
- number of sessions
- length of sessions
- pace of running
- hills
- novel activity
- footware
- ground surface
I think the running pace is the more powerful multiplier in this list. Extra sprint sessions will do it. My kids got sore once when we did a boot-camp session with a novel plyometric exercise - split jumps.
There are also “internal” variables that determine our ability to cope with the training load:
- nutrition
- stress
- sleep
- growth spurts
My kids definitely are more prone to Sever’s if they’ve had a couple of late nights that week. And, if they’re having a growth spurt, their bodies are busy spending resources on growing rather than recovering from the stress of a training session.
NATURAL RECOVERY
Text books say that Sever’s disease is self-limiting because the growth plate eventually fuses by the age of 15 or 16. But I don’t think there’s anyone who would be happy to just let it run its course until then. It is usually sore enough to stop you participating in sport, so it needs treatment.
WHAT DO WE DO?
I used to put kids with heel pain in orthotics, until I read this research which confirms that a simple heel wedge is more effective than orthotics for Sever’s disease. Cheaper and easier, so that's a win.
I get them to do an isometric Achilles strengthening program which also helps with pain control.
But ultimately recovery comes down to load management.
Load management means reducing the excessive loads. So this could be:
And aid recovery with:
I get them to do an isometric Achilles strengthening program which also helps with pain control.
But ultimately recovery comes down to load management.
Load management means reducing the excessive loads. So this could be:
- less sessions/week
- shorter sessions
- less sprint work
- run in joggers rather than spikes or footy boots
- less hills
- heel wedges in shoes
- stay in shoes - no bare feet / thongs / flats. I really like them to stay in some sort of shoe with a heel all the time. Even if they’re getting up to use the bathroom I want them to slip their joggers on.
And aid recovery with:
- plenty of sleep
- massage calf muscles
- ice and Ibuprofen for pain relief when sore
HAVE YOU HAD A CHILD WITH SEVER’S DISEASE?
- Smart mouthguard the new weapon in rugby concussion -
- Athletes struggling with contraceptives and menstrual health as periods remain taboo in sport -
- I want to eat healthily. So why do I crave sugar, salt and carbs? -
- "Naked carbs" and "net carbs" - what are they and should you count them? -
- High Intensity Exercise Can Reverse Neurodegeneration in Parkinson's Disease -
- Inside the brain of a suspected CTE patient -
- Gradual acceptance of concussion risk prompts new reality for Australian sport -

Benign paroxysmal positional vertigo (BPPV) is one of the most common forms of vertigo, affecting 2% of the population at some point in our lives.
BPPV is caused by a problem with the inner ear, where a small calcium deposit forms and moves with gravity around the different angled canals of the inner ear. BPPV is “positional” as it is triggered by specific head movements, for example, turning your head to the left with rolling over in bed. Symptoms of vertigo are room spinning, disturbed balance, and nausea.
BPPV typically resolves within a few weeks, but can be recurring.
Your GP can give you anti-nausea medication, and Physiotherapists treat BPPV with a sequence of movements and positions, called the Epley Manoeuvre, that uses gravity to re-position the calcium crystals.
A video of the Dix Hallpike test for BPPV is HERE.
Information on the Epley Manoeuvre is HERE.
A video of the Epley Manoeuvre is HERE.
Do you have vertigo? Book a physiotherapy appointment in Mosman to perform the Epley Manoeuvre HERE.
BPPV is caused by a problem with the inner ear, where a small calcium deposit forms and moves with gravity around the different angled canals of the inner ear. BPPV is “positional” as it is triggered by specific head movements, for example, turning your head to the left with rolling over in bed. Symptoms of vertigo are room spinning, disturbed balance, and nausea.
BPPV typically resolves within a few weeks, but can be recurring.
Your GP can give you anti-nausea medication, and Physiotherapists treat BPPV with a sequence of movements and positions, called the Epley Manoeuvre, that uses gravity to re-position the calcium crystals.
A video of the Dix Hallpike test for BPPV is HERE.
Information on the Epley Manoeuvre is HERE.
A video of the Epley Manoeuvre is HERE.
Do you have vertigo? Book a physiotherapy appointment in Mosman to perform the Epley Manoeuvre HERE.
- Can kimchi really help you lose weight? -
- How exercise can treat and prevent common mental health issues -
- Can Strength Training Protect You From Running Injuries? -
- Running or Yoga can help beat depression -
- Many of the supposed benefits of sauna and ice baths are not backed by solid evidence -
- Is it broken? A strain or sprain? How to spot a serious injury -
- How long does back pain last? And how can learning about pain increase the chance of recovery? -
- Concussion in sport: why making players sit out for 21 days afterwards is a good idea -
- How much weight do you actually need to lose? It might be a lot less than you think -
- Fempro Armour looks to minimise sporting injuries among women -
- NRL concussion revolution: Contact training limit on cards -
- How long does low back pain last and what treatments can help? -
- Why the biggest threat to the Matildas' knees is sitting on a plane -
- How women respond to strength training -
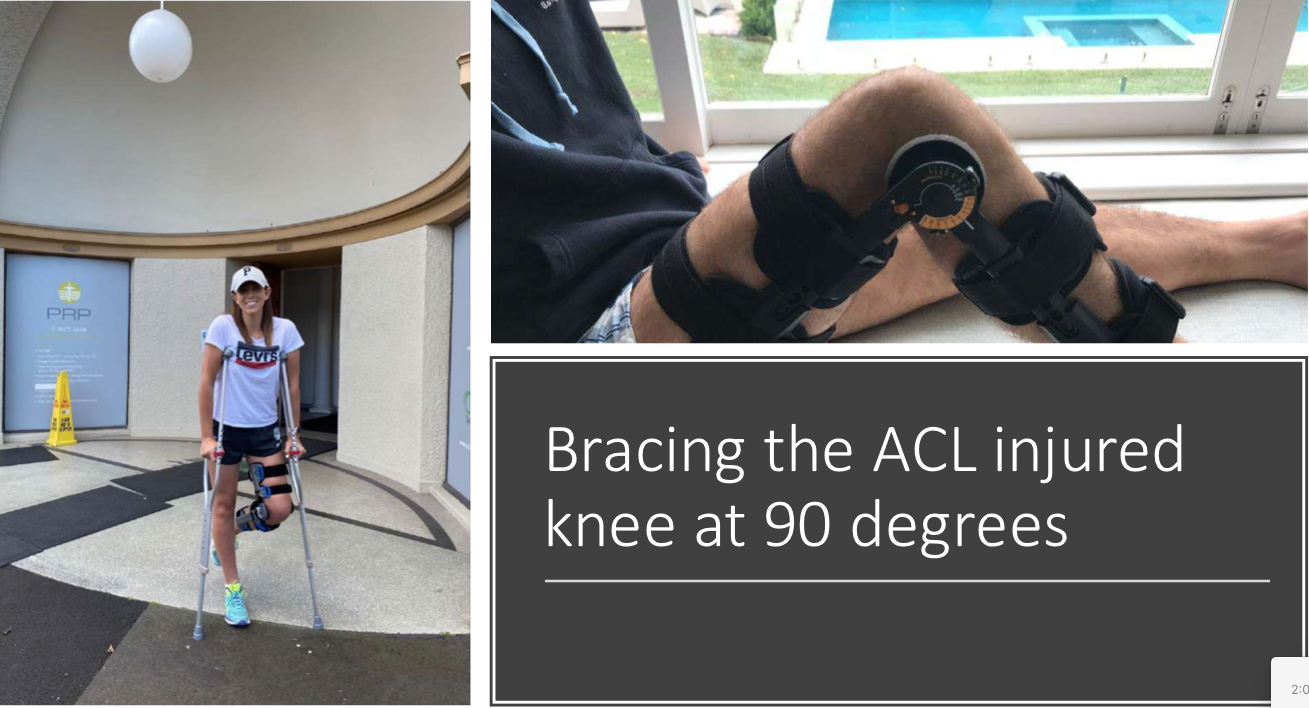
The ACL Cross Bracing Protocol was developed by orthopaedic surgeon, Merv Cross OAM, and his son, Dr Tom Cross, at The Stadium Clinic in Sydney. The novel concept is to heal a ruptured ACL by bracing the injured knee at 90°, a position that most closely approximates the two ends of the torn ACL. The injured ACL heals, negating the need to replace the ACL with reconstructive surgery.
The Cross Bracing Protocol's first patient to achieve a successful healing of their ruptured ACL was a 19 year old netballer in 2014. A case series of the first 80 patients to follow the protocol was published in June, 2023:
90% of the participants (72 of the initial 80) had signs of ACL healing on 3-month MRI. As of October 2023, there are 487 patients and counting. 284 of the first 301 participants (94%) have achieved ACL healing. There are already more than 100 participants > 2 years post-injury. Currently (only) 11% of ACL Cross Bracing Protocol patients have experienced a re-rupture.
The published protocol is here: ACL Cross Bracing Protocol
Since publishing, the protocol has evolved to include more strengthening exercises at an earlier stage, as well as 6-week, and 8-week variations.
As of October 2023, some key points of the protocol are:
DAY OF INJURY:
Features that determine if the ACL Cross Bracing Protocol is appropriate:
If the Cross Bracing Protocol is appropriate...
4-7 DAYS POST INJURY:
The Cross Bracing Protocol's first patient to achieve a successful healing of their ruptured ACL was a 19 year old netballer in 2014. A case series of the first 80 patients to follow the protocol was published in June, 2023:
90% of the participants (72 of the initial 80) had signs of ACL healing on 3-month MRI. As of October 2023, there are 487 patients and counting. 284 of the first 301 participants (94%) have achieved ACL healing. There are already more than 100 participants > 2 years post-injury. Currently (only) 11% of ACL Cross Bracing Protocol patients have experienced a re-rupture.
- There is a very useful website to help promote the novel concept at healacl.com
- There is a Facebook group of participants at "CBP Bracing Pioneers" Community
- A Patient's Story: The Cross Bracing Protocol
The published protocol is here: ACL Cross Bracing Protocol
Since publishing, the protocol has evolved to include more strengthening exercises at an earlier stage, as well as 6-week, and 8-week variations.
As of October 2023, some key points of the protocol are:
DAY OF INJURY:
- First-aid instructions are here
- Range of Motion brace set to 30°-90°
- NWB on crutches
- Arrange for an "emergency" X-ray and MRI, specifically requesting a full sequence / double oblique sequence
with slices no greater than 3mm. PRP Radiology at The Stadium Clinic reserve emergency MRI slots for ACL ruptures. - If in pain, use paracetamol. Avoid anti-inflammatories (NSAIDS) such as Nurofen.
- Arrange appointment with Dr Tom Cross to assess the MRI to decide if the Cross Bracing Protocol is appropriate.
Features that determine if the ACL Cross Bracing Protocol is appropriate:
- 4-7 days post injury
- Gap distance between torn ACL tissue < 4-6mm (depending on patient height)
- No ACL tissue displaced outside the intercondylar notch
- Intact femoral origin of ACL
If the Cross Bracing Protocol is appropriate...
4-7 DAYS POST INJURY:
- Brace fitting. (Dr Cross recommends a Bauerfiend SecuTec Genu Brace with additional 90° extension blocks that must be specifically requested.) I can supply and fit these braces.
- Anti-coagulant medication to mitigate risk of DVT for the first 60 days
- Brace fixed at 90°, 24-hours/day
- NWB on crutches or scooter
- Weekly Physio for exercise progressions from Week 1 -12
- Brace 60°-90° NWB
- Can commence swimming in brace
- Brace 45°-90° NWB
- Brace 30°-140° WBAT
- Can commence stationary bike
- Brace 20°-140° FWB
- Brace 10°-140° FWB
- Brace 0°-140° FWB
- Out of brace (still bracing for crowds / risky situations)
- MRI to assess ACL healing
- Open chain seated leg extensions
- Graded running program
- Agility
- Return to training
- RETURN TO PLAY

- Six surprising things about placebos -
- How do I make sure my child's school backpack is safe? -
- Running's Latest Secret Brain Ingredient is Oxytocin -
- Why more women are flocking to weights rooms and gyms for strength training -
- Longer term impact of sport-related brain injuries revealed -
- A new government inquiry will examine women's pain and treatment -
- The importance of exercise during pregnancy -
- Why Endurance Athletes Are Scarfing Down More Carbs than Ever -
- Why are my muscles sore after exercise? -
- How little strength training can you get away with? -
- Why you shouldn't let guilt motivate you to exercise -
- Thinking of using as activity tracker to achieve your exercise goals? -
- Most Supplements Don't Work -
- Your body has a built in weight loss system -
- You can now order all kinds of medical tests online -
Osteoarthritis (OA) is a leading and increasing cause of disability and has a significant impact on health-related quality of life. Osteoarthritis is a structural change to the cartilage and boney surfaces in a synovial joint. Most of the joints in our skeletal system are synovial joints, which is where two opposing bones articulate in a joint capsule filled with synovial fluid. The synovial fluid is a lubricant to help the joint move, as well as a source of nutrition for the cartilage that lines the joint surfaces. The articulating surfaces in synovial joints are lined with articular cartilage, which is a smooth, glossy surface to decrease the friction in the joint (as opposed to fibrous cartilage, which is the rubbery type cartilage that plays a more structural role, found in the meniscus in knees and the rubbery part of your ribs, nose, and ears).
The fleshy parts of muscles and organs is pink because it is full of blood, which brings oxygen and nutrition, and is important for healing damage. Cartilage looks white because it doesn’t have a blood supply, so articular cartilage relies of the synovial fluid for its nutrition. This isn’t as effective as having a blood supply, so when cartilage is damaged it doesn’t heal well. Nanna damages the cartilage in her knees and it never really repairs.
Once articular cartilage is damaged, the joint tries to reinforce and repair the damaged area by laying down new tissue. It would be great if cartilage repaired itself with new cartilage cells, but the joint wants to make itself even stronger than the obviously insufficient cartilage, so it lays down a stronger building block - bone cells. So when we say that Nanna has “worn away” her knee to the point where it’s “bone on bone”, it’s not just that she’s warn away the cartilage, but actually there’s also a build up of “extra” bone, as the knee tries to make itself stronger than cartilage. Rather than being a nice smooth, glossy surface, the extra bone is now a bit rough, so we can hear and feel some gravely crunching and creaking in an osteoarthritic joint.
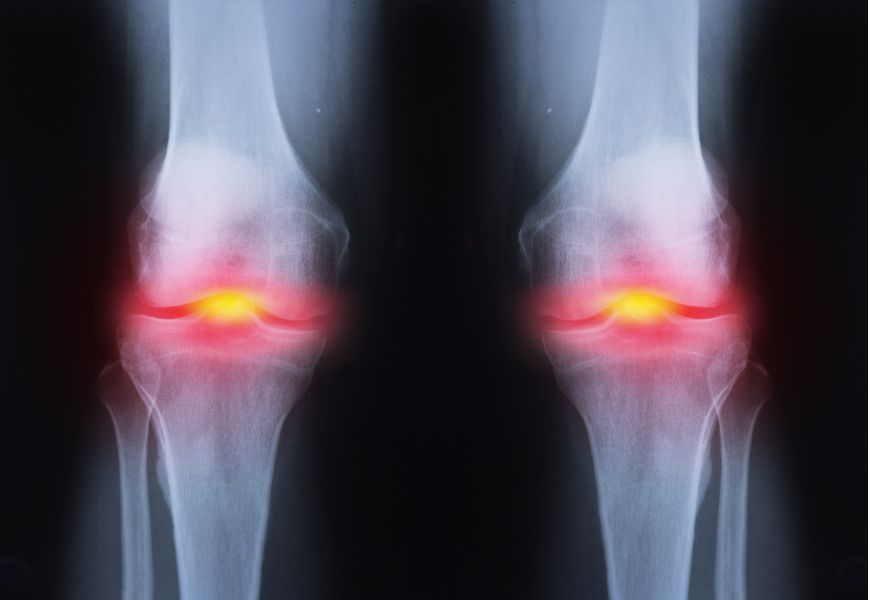
Osteoarthritis occurs most frequently in the knees, hips, hands, and spine and is more common the older we get. Osteoarthritis is diagnosed with an X-ray that shows the changes to the bony profile in the joint.
When we look at what causes osteoarthritis:
Osteoarthritis isn't painful most of the time. At a certain age, essentially everyone will have arthritic changes in their joints without knowing about it. When we X-ray the joint, it doesn’t look as good as it used to, but it doesn’t hurt. It’s a bit like my grey hair and wrinkles - they don’t look great anymore, and it's a sign that I’m getting older, but I don’t expect them to be painful.
If an arthritic joint is painful, it tends to go through phases of being sore and not being sore at all. It can be sore for a day, a week, a month, or a year, but then will be fine again. Whether or not it is sore is not determined by the severity of the changes we see on the X-ray. We can see nasty looking joints that have never been sore, and we see very sore joints that look fine on the X-ray. There isn’t much of a correlation.
What determines whether or not the osteoarthritis hurts is the body’s perception of "vulnerability" in that joint - essentially whether or not it feels strong or weak. Pain is an alarm system “software”, employed to defend against damage to the "hardware”. We can have different levels of sensitivity of how easily the alarm is triggered. Very commonly, an arthritic joint starts to hurt more after a period of rest, as the body looses some fitness, muscles loose some strength, an arthritic joint gets less support from the external scaffolding of the muscles, it feels more vulnerable, and communicates that by being painful, as a way of saying “be careful”.
So that gives us some treatment options for arthritis:
WEIGHT LOSS (Adipose)
EXERCISE
PAIN RELIEF
SURGERY
How do you decide when it’s time to have a joint replacement?
I suggest it’s time when you really can’t walk anymore because of the pain, and/or the pain is stopping you sleeping at night. Joint replacements last for about 25 years on average, so don’t rush into doing it too early. The rehab after surgery is 3-12 months before the leg completely feels like it’s yours. The joint replacements are good for relieving pain, but unfortunately we don’t see improvements in patients’ activity levels after surgery. Total hip replacements are easier all around than total knee replacements.
Do you have Osteoarthritis?
The fleshy parts of muscles and organs is pink because it is full of blood, which brings oxygen and nutrition, and is important for healing damage. Cartilage looks white because it doesn’t have a blood supply, so articular cartilage relies of the synovial fluid for its nutrition. This isn’t as effective as having a blood supply, so when cartilage is damaged it doesn’t heal well. Nanna damages the cartilage in her knees and it never really repairs.
Once articular cartilage is damaged, the joint tries to reinforce and repair the damaged area by laying down new tissue. It would be great if cartilage repaired itself with new cartilage cells, but the joint wants to make itself even stronger than the obviously insufficient cartilage, so it lays down a stronger building block - bone cells. So when we say that Nanna has “worn away” her knee to the point where it’s “bone on bone”, it’s not just that she’s warn away the cartilage, but actually there’s also a build up of “extra” bone, as the knee tries to make itself stronger than cartilage. Rather than being a nice smooth, glossy surface, the extra bone is now a bit rough, so we can hear and feel some gravely crunching and creaking in an osteoarthritic joint.
Osteoarthritis occurs most frequently in the knees, hips, hands, and spine and is more common the older we get. Osteoarthritis is diagnosed with an X-ray that shows the changes to the bony profile in the joint.
When we look at what causes osteoarthritis:
- The biggest contributor is a previous traumatic injury that has physically damaged the cartilage. This can be a landing/twisting injury or sprain, where the trauma of knocking one bone against the other, takes a “divot” or tear in the cartilage, or bruises the cartilage and underlying bone.
- The second biggest cause of osteoarthritis is genetic - the way our joints age, based on our family history. Nanna had a hip replacement and so will I.
- The third biggest contributor to osteoarthritis is BMI. Every 5 kg of weight gain, confers a 36% increase in the risk of OA. Interestingly, it isn’t the extra pressure through the joints of being heavy that causes a problem - fat people have a higher rate of hand osteoarthritis too (which are non weight-bearing joints). The problem with BMI is the systemic inflammatory effect of cytokines produced by fat tissue. Being fat causes inflammation that irritates joints, so fat people get osteoarthritis (and have heart attacks from the scarring/hardening of coronary arteries, also as a reaction to systemic inflammation caused by adipose tissue).
Osteoarthritis isn't painful most of the time. At a certain age, essentially everyone will have arthritic changes in their joints without knowing about it. When we X-ray the joint, it doesn’t look as good as it used to, but it doesn’t hurt. It’s a bit like my grey hair and wrinkles - they don’t look great anymore, and it's a sign that I’m getting older, but I don’t expect them to be painful.
If an arthritic joint is painful, it tends to go through phases of being sore and not being sore at all. It can be sore for a day, a week, a month, or a year, but then will be fine again. Whether or not it is sore is not determined by the severity of the changes we see on the X-ray. We can see nasty looking joints that have never been sore, and we see very sore joints that look fine on the X-ray. There isn’t much of a correlation.
What determines whether or not the osteoarthritis hurts is the body’s perception of "vulnerability" in that joint - essentially whether or not it feels strong or weak. Pain is an alarm system “software”, employed to defend against damage to the "hardware”. We can have different levels of sensitivity of how easily the alarm is triggered. Very commonly, an arthritic joint starts to hurt more after a period of rest, as the body looses some fitness, muscles loose some strength, an arthritic joint gets less support from the external scaffolding of the muscles, it feels more vulnerable, and communicates that by being painful, as a way of saying “be careful”.
So that gives us some treatment options for arthritis:
WEIGHT LOSS (Adipose)
- We know that a 5kg reduction in weight over a 10-year period decreased the likelihood of symptomatic knee OA by 50%.
- Losing 5% of body weight has been shown to provide some pain relief, and 10% provides significant reductions in pain.
EXERCISE
- Stay as active as possible. Rest doesn’t help. Improve muscle mass and strength so the joint is more supported and feels less vulnerable.
- Both aerobic walking and quadriceps' strengthening exercises have been shown to reduce pain and disability in subjects with knee OA.
PAIN RELIEF
- Paracetamol.
- Hot packs.
- Taping.
- Sleeves.
SURGERY
- There’s a lot of research showing that “tidy up” operations, or arthroscopic surgery for osteoarthritis is no better than an exercise program. It’s the exercise you do after the surgery that provides more benefit than the surgery itself.
- For people that never get on top of their arthritis with weight loss and exercise, the pain can get so severe that they end up needing a total joint replacement, where the bones are cut out and replaced with an artificial, metal and plastic joint.
How do you decide when it’s time to have a joint replacement?
I suggest it’s time when you really can’t walk anymore because of the pain, and/or the pain is stopping you sleeping at night. Joint replacements last for about 25 years on average, so don’t rush into doing it too early. The rehab after surgery is 3-12 months before the leg completely feels like it’s yours. The joint replacements are good for relieving pain, but unfortunately we don’t see improvements in patients’ activity levels after surgery. Total hip replacements are easier all around than total knee replacements.
Do you have Osteoarthritis?
- The First Rule of Running After Childbirth -
- Class action claims AFL knew of concussion management risks in 1993 -
- I'm trying to lose weight and eat healthily. Why do I feel so hungry all the time? -
- England's new tackle height laws could change the face of NRL -
- Tackle height debate hits Australian rugby league -
- AFL urged to limit contact training sessions -
- Most concussions don't happen on the sports field -
- Returning to sport postpartum -
- New research has found an existing drug could help many people with painful hand osteoarthritis -
- How 22 minutes of exercise use a day could reduce the health risks from sitting too long -
- Can I actually target areas to lose fat, like my belly? -
- Sports Medicine Australia's expert guide to long-distance running -
- Getting Strong is Good forYour Brain, Even if You Don't Bulk Up -
- What Makes Training High Quality? -
- People with private health insurance save the government $550 a year -
- World Rugby to adopt G-force tech to flag head impacts -
- Nike V Adidas: the battle to create the ultimate "super shoe" -
- What is the OMAD Diet? -
- Worried about getting injured riding a mountain bike? -
- Treadmill, exercise bike, rowing machine: what's the best option for cardio at home? -
- Can coffee help you avoid weight gain? -
- AI and smart mouthguard: the new frontline in fight against brain injuries -
- Adidas' new record-breaking marathon super shoe takes technological arms race to new level -
- The Relationship Between Neck Strength and Sports-Related Concussion in Team Sports -
- Fixing concussion rules in amateur sports will be a 'huge challenge' -
- Breasts are still a taboo topic for women in sport, but plenty can be done to protect them -
- Brain biometrics help identify sports concussions -
�
Archives
May 2024
April 2024
March 2024
February 2024
January 2024
December 2023
November 2023
October 2023
September 2023
August 2023
July 2023
June 2023
May 2023
April 2023
March 2023
February 2023
January 2023
December 2022
November 2022
October 2022
September 2022
August 2022
July 2022
June 2022
May 2022
April 2022
March 2022
February 2022
January 2022
December 2021
November 2021
October 2021
September 2021
August 2021
July 2021
June 2021
May 2021
April 2021
March 2021
February 2021
January 2021
December 2020
November 2020
October 2020
September 2020
August 2020
July 2020
June 2020
May 2020
April 2020
March 2020
February 2020
December 2019
November 2019
October 2019
September 2019
August 2019
July 2019
June 2019
May 2019
April 2019
March 2019
January 2019
December 2018
November 2018
October 2018
September 2018
August 2018
July 2018
June 2018
May 2018
April 2018
March 2018
February 2018
January 2018
December 2017
November 2017
October 2017
September 2017
August 2017
July 2017
June 2017
May 2017
April 2017
March 2017
February 2017
January 2017
December 2016
November 2016
May 2016
November 2015
October 2015
September 2015
August 2015
July 2015
June 2015
May 2015
Categories
All
Achilles
ACL
Active Transport
Acupuncture
Ageing
AHPRA
Alcohol
Ankle
Ankylosing Spondylitis
Apps
Arthritis
Arthroscopy
Babies
Backpacks
Back Pain
Blood Pressure
BMI
Body Image
Bunions
Bursitis
Cancer
Chiro
Chiropractic
Cholesterol
Chronic Pain
Concussion
Copenhagen
Costochondritis
Cramp
Crossfit
Cycling
Dance
Dementia
Depression
De Quervains
Diet
Dieting
Elbow
Exercise
Falls
Fat
Feet
Fibromyalgia
Fibula
Finger
Fitness Test
Food
Foot
Fracture
Fractures
Glucosamine
Golfers Elbow
Groin
GTN
Hamstring
Health
Heart-disease
Heart-failure
Heat
HIIT Training
Hip-fracture
Hydration
Hyperalgesia
Ibuprofen
Injections
Injury
Injury Prevention
Isometric Exercise
Knee
Knee Arthroscopy
Knee Replacement
Knees
LARs Ligament Reconstruction
Lisfranc
Load
Low Back Pain
Massage
Meditation
Meniscus
Minimalist Shoes
MRI
MS
Multiple Sclerosis
Netball
Nutrition
OA
Obesity
Orthotics
Osgood-Schlatter
Osteoarthritis
Osteopath
Osteoperosis
Pain
Parkinsons
Patella
Peroneal-tendonitis
Physical-activity
Physio
Physio Mosman
Pigeon-toed
Pilates
Piriformis
Pokemon
Posture
Prehab
Prolotherapy
Pronation
PRP
Radiology
Recovery
Rehab
Rheumatoid
Rheumatoid-arthritis
Rotator Cuff
RTP
Rugby
Running
Running Shoes
Scan
Severs
Shin-pain
Shoes
Shoulder
Shoulder Dislocation
Sitting
Sleep
Soccer
Spinal-fusion
Spondyloarthritis
Spondylolisthesis
Sports Injury
Sports Physio
Standing
Standing-desk
Statins
Stem-cells
Stress Fracture
Stretching
Sugar
Supplements
Surgery
Sweat
Tendinopathy
Tendinosis
Tendonitis
Tmj
Treatment
Vertigo
Walking
Warm-Up
Weight Loss
Wheezing
Whiplash
Wrist
Yoga
 RSS Feed
RSS Feed